Nail clubbing

 Clash Royale CLAN TAG#URR8PPP
Clash Royale CLAN TAG#URR8PPP
This article's lead section may not adequately summarize its contents. (November 2018) |
| Clubbing | |
|---|---|
| Synonyms | Drumstick fingers, digital clubbing, watch-glass nails[1] |
 | |
| Clubbing | |
| Specialty | Pulmonology |
Nail clubbing, also known as digital clubbing, is a deformity of the finger or toe nails associated with a number of diseases, mostly of the heart and lungs.[2][3] Clubbing for no obvious reason can also occur, but is rare.[4][5]Hippocrates was the first to formally document clubbing as a sign of disease, and the phenomenon is therefore occasionally called "Hippocratic fingers."
Contents
1 Causes
1.1 Isolated clubbing
1.2 HPOA
1.3 Primary HPOA
2 Pathophysiology
3 Diagnosis
3.1 Detection
4 Epidemiology
5 See also
6 References
7 External links
Causes
Isolated clubbing
Clubbing is associated with:
- Lung disease:
Lung cancer, mainly non-small-cell (54% of all cases), not seen frequently in small-cell lung cancer (< 5% of cases)[6]
Interstitial lung disease most commonly idiopathic pulmonary fibrosis- Complicated tuberculosis
- Suppurative lung disease: lung abscess, empyema, bronchiectasis, cystic fibrosis
Mesothelioma of the pleura- Arteriovenous fistula or malformation
- Sarcoidosis
- Heart disease:
- Any disease featuring chronic hypoxia
- Congenital cyanotic heart disease (most common cardiac cause)
- Subacute bacterial endocarditis
Atrial myxoma (benign tumor)- Tetralogy of Fallot
- Any disease featuring chronic hypoxia
- Gastrointestinal and hepatobiliary:
- Malabsorption
Crohn's disease and ulcerative colitis
Cirrhosis, especially in primary biliary cirrhosis[7]
Hepatopulmonary syndrome, a complication of cirrhosis[8]
- Others:
Graves' disease (autoimmune hyperthyroidism) – in this case it is known as thyroid acropachy[9]- Familial and racial clubbing and "pseudoclubbing" (people of African descent often have what appears to be clubbing)
- Vascular anomalies of the affected arm such as an axillary artery aneurysm (in unilateral clubbing)
Nail clubbing is not specific to chronic obstructive pulmonary disease (COPD). Therefore, in patients with COPD and significant degrees of clubbing, a search for signs of bronchogenic carcinoma (or other causes of clubbing) might still be indicated.[10]
A congenital form has also been recognized.[11]
HPOA

Bone scan of a patient with HPOA
A special form of clubbing is hypertrophic pulmonary osteoarthropathy, known in continental Europe as Pierre Marie-Bamberger syndrome. This is the combination of clubbing and thickening of periosteum (connective tissue lining of the bones) and synovium (lining of joints), and is often initially diagnosed as arthritis. It is commonly associated with lung cancer.[citation needed]
Primary HPOA
Primary hypertrophic osteoarthropathy is HPOA without signs of pulmonary disease. This form has a hereditary component, although subtle cardiac abnormalities can occasionally be found. It is known eponymously as the Touraine–Solente–Golé syndrome. This condition has been linked to mutations in the gene on the fourth chromosome (4q33-q34) coding for the enzyme 15-hydroxyprostaglandin dehydrogenase (HPGD); this leads to decreased breakdown of prostaglandin E2 and elevated levels of this substance.[12]
Pathophysiology
The exact cause for sporadic clubbing is unknown, with numerous theories as to its cause. Vasodilation (i.e., distended blood vessels), secretion of growth factors (e.g., platelet-derived growth factor and hepatocyte growth factor) from the lungs, and other mechanisms have been proposed. The discovery of disorders in the prostaglandin metabolism in primary osteoarthropathy has led to suggestions that overproduction of PGE2 by other tissues may be the causative factor for clubbing.[12]
Another mechanism by which clubbing is thought to arise from is due to increased entry of megakaryocytes into the systemic circulation. Under normal circumstances in healthy individuals, megakaryocytes that arise from the bone marrow are trapped in the pulmonary capillary bed and broken down before it enters the systemic circulation. It is thought that in disorders where there is right-to-left shunting or lung malignancy, the megakaryocytes can bypass the breakdown within the pulmonary circulation and enter the systemic circulation. They are then trapped within the capillary beds within the extremities, such as the digits, and release platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF). PDGF and VEGF have growth promoting properties and causes connective tissue hypertrophy and capillary permeability.[13]
Diagnosis
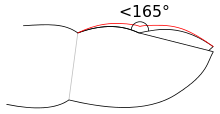
Clubbing of the fingernail: The red line shows the outline of a clubbed nail.
When clubbing is encountered in patients, doctors will seek to identify its cause and exclude pseudoclubbing before making the diagnosis. They usually accomplish this by obtaining a detailed medical history—particular attention is paid to lung, heart, and gastrointestinal conditions—and conducting a thorough clinical examination, which may disclose associated features relevant to the underlying diagnosis. Additional studies such as a chest X-ray and a chest CT-scan may also be performed.[10]
Detection
Clubbing may be present in one of five stages:[10]
No visible clubbing - Fluctuation (increased ballotability) and softening of the nail bed only. No visible changes of nails.
Mild clubbing - Loss of the normal <165° angle (Lovibond angle) between the nailbed and the fold (cuticula). Schamroth's window (see below) is obliterated. Clubbing is not obvious at a glance.
Moderate clubbing - Increased convexity of the nail fold. Clubbing is apparent at a glance.
Gross clubbing - Thickening of the whole distal (end part of the) finger (resembling a drumstick)
Hypertrophic osteoarthropathy - Shiny aspect and striation of the nail and skin
Schamroth's test or Schamroth's window test (originally demonstrated by South African cardiologist Leo Schamroth on himself)[14] is a popular test for clubbing. When the distal phalanges (bones nearest the fingertips) of corresponding fingers of opposite hands are directly opposed (place fingernails of same finger on opposite hands against each other, nail to nail), a small diamond-shaped "window" is normally apparent between the nailbeds. If this window is obliterated, the test is positive and clubbing is present.

Severe clubbing

Front view

Side views

Cyanotic nail beds




Epidemiology
The exact frequency of clubbing in the population is not known. A 2008 study found clubbing in 1%, or 15 patients, of 1511 patients admitted to a department of internal medicine in Belgium. Of these, 40%, or 6 patients, turned out to have significant underlying disease of various causes, while 60%, or 9 patients, had no medical problems on further investigations and remained well over the subsequent year.[5]
See also
Clubbed thumb (unrelated congenital deformity)
References
^ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0..mw-parser-output cite.citationfont-style:inherit.mw-parser-output .citation qquotes:"""""""'""'".mw-parser-output .citation .cs1-lock-free abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .citation .cs1-lock-limited a,.mw-parser-output .citation .cs1-lock-registration abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .citation .cs1-lock-subscription abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registrationcolor:#555.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration spanborder-bottom:1px dotted;cursor:help.mw-parser-output .cs1-ws-icon abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/4/4c/Wikisource-logo.svg/12px-Wikisource-logo.svg.png")no-repeat;background-position:right .1em center.mw-parser-output code.cs1-codecolor:inherit;background:inherit;border:inherit;padding:inherit.mw-parser-output .cs1-hidden-errordisplay:none;font-size:100%.mw-parser-output .cs1-visible-errorfont-size:100%.mw-parser-output .cs1-maintdisplay:none;color:#33aa33;margin-left:0.3em.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-formatfont-size:95%.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-leftpadding-left:0.2em.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-rightpadding-right:0.2em
^ Rutherford, JD (14 May 2013). "Digital clubbing". Circulation. 127 (19): 1997–9. doi:10.1161/circulationaha.112.000163. PMID 23671180.
^ Freedberg, et al. (2003). Fitzpatrick's Dermatology in General Medicine. (6th ed.). McGraw-Hill.
ISBN 0-07-138076-0. :656
^ Schwatz, RA. "Clubbing of the Nails". Medscape. Medscape. Retrieved 14 August 2014.
^ ab Vandemergel X, Renneboog B (July 2008). "Prevalence, aetiologies and significance of clubbing in a department of general internal medicine". Eur. J. Intern. Med. 19 (5): 325–9. doi:10.1016/j.ejim.2007.05.015. PMID 18549933.
^ Sridhar KS, Lobo CF, Altman RD (1998). "Digital clubbing and lung cancer". Chest. 114 (6): 1535–37. doi:10.1378/chest.114.6.1535. PMID 9872183. Archived from the original (PDF) on 2003-11-01.
^ Epstein O, Dick R, Sherlock S (1981). "Prospective study of periostitis and finger clubbing in primary biliary cirrhosis and other forms of chronic liver disease". Gut. 22 (3): 203–6. doi:10.1136/gut.22.3.203. PMC 1419499. PMID 7227854.
^ Naeije R (March 2003). "Hepatopulmonary syndrome and portopulmonary hypertension". Swiss Med Wkly. 133 (11–12): 163–9. PMID 12715285.
^ "acropachy". GPnotebook.
^ abc Myers KA, Farquhar DR (2001). "The rational clinical examination: does this patient have clubbing?". JAMA. 286 (3): 341–7. doi:10.1001/jama.286.3.341. PMID 11466101.
^ Shah K, Ferrara TM, Jan A, Umair M, Irfanullah, Khan S, Ahmad W, Spritz RA (August 2017). "Homozygous SLCO2A1 translation initiation codon mutation in a Pakistani family with recessive isolated congenital nail clubbing". Br. J. Dermatol. 177 (2): 546–548. doi:10.1111/bjd.15094. PMID 27681482.
^ ab Uppal S, Diggle CP, Carr IM, et al. (June 2008). "Mutations in 15-hydroxyprostaglandin dehydrogenase cause primary hypertrophic osteoarthropathy". Nat. Genet. 40 (6): 789–93. doi:10.1038/ng.153. PMID 18500342.
^ Dickinson, CJ; Martin, JF (19 December 1987). "Megakaryocytes and platelet clumps as the cause of finger clubbing". Lancet. 2 (8573): 1434–5. PMID 2891996.
^ Schamroth L (February 1976). "Personal experience". S. Afr. Med. J. 50 (9): 297–300. PMID 1265563.
External links
| Classification | D |
|---|
| Classification | D
|
|---|