Glioma

 Clash Royale CLAN TAG#URR8PPP
Clash Royale CLAN TAG#URR8PPP | Glioma | |
|---|---|
 | |
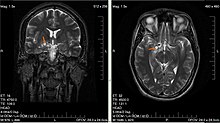
Glioma in the left parietal lobe (brain CT scan), WHO grade 2. | |
| Specialty | Oncology |
A glioma is a type of tumor that starts in the glial cells of the brain or the spine.[1] Gliomas comprise about 30 per cent of all brain tumors and central nervous system tumors, and 80 per cent of all malignant brain tumors.[2]
Contents
1 Classification
1.1 By type of cell
1.2 By grade
1.3 By location
2 Signs and symptoms
3 Causes
4 Pathophysiology
5 Treatment
5.1 Refractory disease
5.2 Relative effectiveness
6 Prognosis
6.1 Low grade
6.2 High grade
6.3 Diffuse intrinsic pontine glioma
6.4 IDH1 and IDH2-mutated glioma
7 References
8 External links
Classification
Gliomas are classified by cell type, by grade, and by location.
By type of cell
Gliomas are named according to the specific type of cell with which they share histological features, but not necessarily from which they originate. The main types of gliomas are:[3]
Ependymomas: ependymal cells
Astrocytomas: astrocytes (glioblastoma multiforme is a malignant astrocytoma and the most common primary brain tumor among adults).
Oligodendrogliomas: oligodendrocytes
Brainstem glioma: develop in the brain stem- Optic nerve glioma: develop in or around the optic nerve
- Mixed gliomas, such as oligoastrocytomas, contain cells from different types of glia
By grade
Gliomas are further categorized according to their grade, which is determined by pathologic evaluation of the tumor. The neuropathological evaluation and diagnostics of brain tumor specimens is performed according to WHO Classification of Tumours of the Central Nervous System.[4][5]
Low-grade brain glioma in a 28-year-old male. (Taken on 10 July 2007)
- Low-grade gliomas [WHO grade II] are well-differentiated (not anaplastic); these tend to exhibit benign tendencies and portend a better prognosis for the patient. However, they have a uniform rate of recurrence and increase in grade over time so should be classified as malignant.
- High-grade [WHO grades III–IV] gliomas are undifferentiated or anaplastic; these are malignant and carry a worse prognosis.
Of numerous grading systems in use, the most common is the World Health Organization (WHO) grading system for astrocytoma, under which tumors are graded from I (least advanced disease—best prognosis) to IV (most advanced disease—worst prognosis).
By location
Gliomas can be classified according to whether they are above or below a membrane in the brain called the tentorium. The tentorium separates the cerebrum (above) from the cerebellum (below).
- The supratentorial is above the tentorium, in the cerebrum, and mostly found in adults (70%).
- The infratentorial is below the tentorium, in the cerebellum, and mostly found in children (70%).
- The pontine tumors are located in the pons of the brainstem. The brainstem has three parts (pons, midbrain, and medulla); the pons controls critical functions such as breathing, making surgery on these extremely dangerous.
Signs and symptoms
Symptoms of gliomas depend on which part of the central nervous system is affected. A brain glioma can cause headaches, vomiting, seizures, and cranial nerve disorders as a result of increased intracranial pressure. A glioma of the optic nerve can cause visual loss. Spinal cord gliomas can cause pain, weakness, or numbness in the extremities. Gliomas do not metastasize by the bloodstream, but they can spread via the cerebrospinal fluid and cause "drop metastases" to the spinal cord.
A child who has a subacute disorder of the central nervous system that produces cranial nerve abnormalities (especially of cranial nerve VII and the lower bulbar nerves), long-tract signs, unsteady gait secondary to spasticity, and some behavioral changes is most likely to have a pontine glioma.[6]
Causes
The exact causes of gliomas are not known. Hereditary genetic disorders such as neurofibromatoses (type 1 and type 2) and tuberous sclerosis complex are known to predispose to their development.[7] Different oncogenes can cooperate in the development of gliomas.[8]
Some studies of diet and vitamin supplementation seem to indicate that dietary N-nitroso compounds might influence the risk of both childhood and adult brain tumors. Researchers have observed in some studies that brain tumor patients (or their mothers) have generally consumed more cured foods (also known as Curing) than control groups. Recently, Drs. Lee, Wrensch and others found that adults with glioma were more likely to consume diets high in cured foods and low in vitamin C-rich fruits and vegetables, and to consume diets high in nitrites and low in vitamin C. The effect was more pronounced in men than women. However, the pattern of increased risk with increased consumption of cured foods, and decreased risk with greater consumption of fruits, vegetables, and antioxidant vitamins is compatible with other cancer studies that show increased consumption of vegetables and possibly of fruits is associated with decreased cancer risk.[9]
Gliomas have been correlated to the electromagnetic radiation from cell phones, and a link between the cancer and cell phone usage was considered possible,[10] though several large studies have found no conclusive evidence, as summarized by the NIH's National Cancer Institute review of the topic[11] and its numerous citations,[12] and the FCC.[13] However, further research is still being pursued to obtain more robust evidence and verify that there is no relationship (the NIH's National Institute of Environmental Health Sciences most recent press release discussed an ongoing study[14] showing mildly positive results,[15] although it appears there may have been issues with the control group dying prematurely[16]).
Most glioblastomas are infected with cytomegalovirus, which speeds the development of tumors.[17][18][19] Though some studies have shown that farmers have higher rates of gliomas compared to the general population, exposure to farm animals or manure is not associated with glioma.[20][21] Later studies have not found an association between farming and gliomas; similar conflicting data concerns teachers and glioma. More consistent data shows that architects, surveyors, retail workers, butchers, and engineers have higher rates of gliomas.[22] Most studies have found that pesticide exposure is probably not a cause of glioma, though a minority of studies have found an association.[22][23]
Germ-line (inherited) polymorphisms of the DNA repair genes ERCC1, ERCC2 (XPD) and XRCC1 increase the risk of glioma.[24] This indicates that altered or deficient repair of DNA damage contributes to the formation of gliomas. DNA damages are a likely major primary cause of progression to cancer in general.[25] Excess DNA damages can give rise to mutations through translesion synthesis. Furthermore, incomplete DNA repair can give rise to epigenetic alterations or epimutations.[26][27] Such mutations and epimutations may provide a cell with a proliferative advantage which can then, by a process of natural selection, lead to progression to cancer.[25]
Epigenetic repression of DNA repair genes is often found in progression to sporadic glioblastoma. For instance, methylation of the DNA repair gene MGMT promoter was observed in 51% to 66% of glioblastoma specimens.[28][29] In addition, in some glioblastomas, the MGMT protein is deficient due to another type of epigenetic alteration. MGMT protein expression may also be reduced due to increased levels of a microRNA that inhibits the ability of the MGMT messenger RNA to produce the MGMT protein.[29] Zhang et al.[30] found, in the glioblastomas without methylated MGMT promoters, that the level of microRNA miR-181d is inversely correlated with protein expression of MGMT and that the direct target of miR-181d is the MGMT mRNA 3’UTR (the three prime untranslated region of MGMT messenger RNA).
Epigenetic reductions in expression of another DNA repair protein, ERCC1, were found in an assortment of 32 gliomas.[31] For 17 of the 32 (53%) of the gliomas tested, ERCC1 protein expression was reduced or absent. In the case of 12 gliomas (37.5%) this reduction was due to methylation of the ERCC1 promoter. For the other 5 gliomas with reduced ERCC1 protein expression, the reduction could have been due to epigenetic alterations in microRNAs that affect ERCC1 expression.[25]
When expression of DNA repair genes is reduced, DNA damages accumulate in cells at a higher than normal level, and such excess damages cause increased frequencies of mutation.[32][33][34] Mutations in gliomas frequently occur in either isocitrate dehydrogenase (IDH) 1 or 2 genes.[35] One of these mutations (mostly in IDH1) occurs in about 80% of low grade gliomas and secondary high-grade gliomas.[36] Wang et al.[37] pointed out that IDH1 and IDH2 mutant cells produce an excess metabolic intermediate, 2-hydroxyglutarate, which binds to catalytic sites in key enzymes that are important in altering histone and DNA promoter methylation. Thus, mutations in IDH1 and IDH2 generate a “DNA CpG island methylator phenotype or CIMP”[38][39] that causes promoter hypermethylation and concomitant silencing of tumor suppressor genes such as DNA repair genes MGMT and ERCC1. On the other hand, Cohen et al.[36] and Molenaar et al.[35] pointed out that mutations in IDH1 or IDH2 can cause increased oxidative stress. Increased oxidative damage to DNA could be mutagenic. This is supported by an increased number of DNA double-strand breaks in IDH1-mutated glioma cells.[40] Thus, IDH1 or IDH2 mutations act as driver mutations in glioma carcinogenesis, though it is not clear by which role they are primarily acting. A study, involving 51 patients with brain gliomas who had two or more biopsies over time, showed that mutation in the IDH1 gene occurred prior to the occurrence of a p53 mutation or a 1p/19q loss of heterozygosity, indicating that an IDH1 mutation is an early driver mutation.[41]
Pathophysiology
High-grade gliomas are highly vascular tumors and have a tendency to infiltrate. They have extensive areas of necrosis and hypoxia. Often, tumor growth causes a breakdown of the blood–brain barrier in the vicinity of the tumor. As a rule, high-grade gliomas almost always grow back even after complete surgical excision, so are commonly called recurrent cancer of the brain.
Conversely, low-grade gliomas grow slowly, often over many years, and can be followed without treatment unless they grow and cause symptoms.
Several acquired (not inherited) genetic mutations have been found in gliomas. Tumor suppressor protein 53 (p53) is mutated early in the disease.[42] p53 is the "guardian of the genome", which, during DNA and cell duplication, makes sure the DNA is copied correctly and destroys the cell (apoptosis) if the DNA is mutated and cannot be fixed. When p53 itself is mutated, other mutations can survive. Phosphatase and tensin homolog (PTEN), another tumor suppressor gene, is itself lost or mutated. Epidermal growth factor receptor, a growth factor that normally stimulates cells to divide, is amplified and stimulates cells to divide too much. Together, these mutations lead to cells dividing uncontrollably, a hallmark of cancer. Recently, mutations in IDH1 and IDH2 were found to be part of the mechanism and associated with a more favorable prognosis.[43]
Treatment
Treatment for brain gliomas depends on the location, the cell type, and the grade of malignancy. Often, treatment is a combined approach, using surgery, radiation therapy, and chemotherapy. The radiation therapy is in the form of external beam radiation or the stereotactic approach using radiosurgery. Spinal cord tumors can be treated by surgery and radiation. Temozolomide, a chemotherapeutic drug, is able to cross the blood–brain barrier effectively and is currently being used in therapy for high-grade tumors.
Refractory disease
For recurrent high-grade glioblastoma, recent studies have taken advantage of angiogenic blockers such as bevacizumab in combination with conventional chemotherapy, with encouraging results.[44]
Relative effectiveness
A 2017 meta-analysis compared surgical resection versus biopsy as the initial surgical management option for a person with a low-grade glioma.[45] Results show the evidence is insufficient to make a reliable decision.[45] The relative effectiveness of surgical resection compared to biopsy for people with malignant glioma (high-grade) is unknown.[46]
For high-grade gliomas, a 2003 meta-analysis compared radiotherapy with radiotherapy and chemotherapy. It showed a small but clear improvement from using chemotherapy with radiotherapy.[47]
Temozolomide is effective for treating Glioblastoma Multiforme (GBM) compared to radiotherapy alone.[48] A 2013 meta-analysis showed that Temozolomide prolongs survival and delays progression, but is associated with an increase in side effects such as blood complications, fatigue, and infection.[48] For people with recurrent GBM, when comparing temozolomide with chemotherapy, there may be an improvement in the time-to-progression and the person's quality of life, but no improvement in overall survival, with temozolomide treatment.[48]
A mutational analysis of 23 initial-low grade gliomas and recurrent tumors from the same patients has challenged the benefits and usage of Temozolomide. The study showed that when lower grade brain tumors of patients are removed and patients are further treated with Temozolomide, 6 out of 10 times the recurrent tumors were more aggressive and acquired alternative and more mutations.[49] As one of the last authors, Costello, stated "They had a 20- to 50-fold increase in the number of mutations. A patient who received surgery alone who might have had 50 mutations in the initial tumor and 60 in the recurrence. But patients who received TMZ might have 2,000 mutations in the recurrence."[50] Further, new mutations were verified to carry known signatures of Temozolomide induced mutations. The research suggests that Temozolomide for the treatment of certain brain tumors should be thoroughly thought. Unjudicious usage of Temozolomide might lower the prognosis of the patients further, or increase their burden. Further understanding of the mechanisms of Temozolomide induced mutations and novel combination approaches could be promising.
Prognosis
Gliomas are rarely curable. The prognosis for patients with high-grade gliomas is generally poor, and is especially so for older patients. Of 10,000 Americans diagnosed each year with malignant gliomas, about half are alive one year after diagnosis, and 25% after two years. Those with anaplastic astrocytoma survive about three years. Glioblastoma multiforme has a worse prognosis with less than a 12-month average survival after diagnosis, though this has extended to 14 months with more recent treatments.[51]
Low grade
For low-grade tumors, the prognosis is somewhat more optimistic. Patients diagnosed with a low-grade glioma are 17 times as likely to die as matched patients in the general population.[52]
The age-standardized 10-year relative survival rate was 47%.[52] One study reported that low-grade oligodendroglioma patients have a median survival of 11.6 years;[53] another reported a median survival of 16.7 years.[54]
High grade
This group comprises anaplastic astrocytomas and glioblastoma multiforme. Whereas the median overall survival of anaplastic (WHO grade III) gliomas is approximately 3 years, glioblastoma multiforme has a poor median overall survival of c. 15 months.[55]
Diffuse intrinsic pontine glioma
Diffuse intrinsic pontine glioma primarily affects children, usually between the ages of 5 and 7.[56] The median survival time with DIPG is under 12 months.[57] Surgery to attempt tumour removal is usually not possible or advisable for DIPG. By their very nature, these tumours invade diffusely throughout the brain stem, growing between normal nerve cells. Aggressive surgery would cause severe damage to neural structures vital for arm and leg movement, eye movement, swallowing, breathing, and even consciousness.[58][59][unreliable medical source?] Trials of drug candidates have been unsuccessful.[60] The disease is primarily treated with radiation therapy alone.
IDH1 and IDH2-mutated glioma
Patients with glioma carrying mutations in either IDH1 or IDH2 have a relatively favorable survival, compared with patients with glioma with wild-type IDH1/2 genes. In WHO grade III glioma, IDH1/2-mutated glioma have a median prognosis of ~3.5 years, whereas IDH1/2 wild-type glioma perform poor with a median overall survival of c. 1.5 years.[35] In glioblastoma, the difference is larger. There, IDH1/2 wild-type glioblastoma have a median overall survival of 1 year, whereas IDH1/2-mutated glioblastoma have a median overall survival of more than 3 years.[61]
References
^ Mamelak AN, Jacoby DB (March 2007). "Targeted Delivery of Antitumoral Therapy to Glioma and Other Malignancies with Synthetic Chlorotoxin (TM-601)". Expert Opin Drug Deliv. 4 (2): 175–86. doi:10.1517/17425247.4.2.175. PMID 17335414..mw-parser-output cite.citationfont-style:inherit.mw-parser-output qquotes:"""""""'""'".mw-parser-output code.cs1-codecolor:inherit;background:inherit;border:inherit;padding:inherit.mw-parser-output .cs1-lock-free abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .cs1-lock-limited a,.mw-parser-output .cs1-lock-registration abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .cs1-lock-subscription abackground:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registrationcolor:#555.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration spanborder-bottom:1px dotted;cursor:help.mw-parser-output .cs1-hidden-errordisplay:none;font-size:100%.mw-parser-output .cs1-visible-errorfont-size:100%.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-formatfont-size:95%.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-leftpadding-left:0.2em.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-rightpadding-right:0.2em
^ Goodenberger ML, Jenkins RB (2012). "Genetics of adult glioma". Cancer Genet. 205: 613–21. doi:10.1016/j.cancergen.2012.10.009.
^ "Gliomas". Johns Hopkins Medicine Health Library. Retrieved 19 April 2017.
^ Louis, David N.; Perry, Arie; Reifenberger, Guido; Deimling, Andreas von; Figarella-Branger, Dominique; Cavenee, Webster K.; Ohgaki, Hiroko; Wiestler, Otmar D.; Kleihues, Paul (2016-06-01). "The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary". Acta Neuropathologica. 131 (6): 803–820. doi:10.1007/s00401-016-1545-1. ISSN 0001-6322.
^ WHO classification of tumours of the central nervous system. Louis, David N., Ohgaki, Hiroko, Wiestler, O. D. (Otmar D.), 1956-, Cavenee, W. K. (Webster K.),, World Health Organization,, International Agency for Research on Cancer, (Revised 4th ed.). Lyon. ISBN 9789283244929. OCLC 951745876.
^ PRETEST pediatrics p. 224
^ Reuss, D; von Deimling, A (2009). "Hereditary tumor syndromes and gliomas". Recent results in cancer research. Fortschritte der Krebsforschung. Progres dans les recherches sur le cancer. 171: 83–102. doi:10.1007/978-3-540-31206-2_5. PMID 19322539.
^ Radner H, El-Shabrawi Y, Eibl RH, Brüstle O, Kenner L, Kleihues P, Wiestler OD (1993). "Tumor induction by ras and myc oncogenes in fetal and neonatal brain: modulating effects of developmental stage and retroviral dose". Acta Neuropathologica. 86 (5): 456–65. doi:10.1007/bf00228580. PMID 8310796.
^ http://www.kallansklan.org/uploads/FactSheet-WhoGetsBTsv_20rev.pdf
^ "IARC classifies radiofrequency electromagnetic fields as possibly carcinogenic to humans" (PDF) (Press release). IARC. 31 May 2011.
^ "Cell Phones and Cancer Risk". National Cancer Institute. Retrieved 2016-05-29.
^ "Cell Phones and Cancer Risk (References)". National Cancer Institute. Retrieved 2016-05-29.
^ "Wireless Devices and Health Concerns". Federal Communications Commission. 2011-05-26. Retrieved 2016-05-29.
^ "Media Telebriefing: NTP Cell Phone Radiofrequency Radiation Study: Partial Release of Findings". www.niehs.nih.gov. Retrieved 2016-05-29.
^ Wyde, Michael; Cesta, Mark; Blystone, Chad; Elmore, Susan; Foster, Paul; Hooth, Michelle; Kissling, Grace; Malarkey, David; Sills, Robert (2016-05-26). "Report of Partial findings from the National Toxicology Program Carcinogenesis Studies of Cell Phone Radiofrequency Radiation in Hsd: Sprague Dawley® SD rats (Whole Body Exposure)". bioRxiv 055699.
^ Storrs, Storrs. "Cell phone-related cancer for rats raises alarm". CNN.com. Retrieved 2016-05-29.
^ Michaelis M, Baumgarten P, Mittelbronn M, Driever PH, Doerr HW, Cinatl J, Jr (February 2011). "Oncomodulation by human cytomegalovirus: novel clinical findings open new roads". Medical microbiology and immunology. 200 (1): 1–5. doi:10.1007/s00430-010-0177-7. PMID 20967552.CS1 maint: Uses authors parameter (link)
^ Barami, K (July 2010). "Oncomodulatory mechanisms of human cytomegalovirus in gliomas". Journal of Clinical Neuroscience. 17 (7): 819–23. doi:10.1016/j.jocn.2009.10.040. PMID 20427188.
^ Dziurzynski K, Chang SM, Heimberger AB, Kalejta RF, McGregor Dallas SR, Smit M, Soroceanu L, Cobbs CS; HCMV and Gliomas Symposium (Mar 2012). "Consensus on the role of human cytomegalovirus in glioblastoma". Neuro Oncol. 14 (3): 246–55. doi:10.1093/neuonc/nor227. PMC 3280809. PMID 22319219.CS1 maint: Uses authors parameter (link)
^ Efird, Jimmy T.; Davies, Stephen W.; O'Neal, Wesley T.; Anderson, Ethan J. (2014). "Animal viruses, bacteria, and cancer: a brief commentary". Frontiers in Public Health. 2: 14. doi:10.3389/fpubh.2014.00014. ISSN 2296-2565. PMC 3923154. PMID 24592380.
^ Ruder, Avima M.; Carreón, Tania; Butler, Mary Ann; Calvert, Geoffrey M.; Davis-King, Karen E.; Waters, Martha A.; Schulte, Paul A.; Mandel, Jack S.; Morton, Roscoe F. (Jun 15, 2009). "Exposure to farm crops, livestock, and farm tasks and risk of glioma: the Upper Midwest Health Study". American Journal of Epidemiology. 169 (12): 1479–91. doi:10.1093/aje/kwp075. ISSN 1476-6256. PMID 19403843.
^ ab Ostrom, Quinn T.; Bauchet, Luc; Davis, Faith G.; Deltour, Isabelle; Fisher, James L.; Langer, Chelsea Eastman; Pekmezci, Melike; Schwartzbaum, Judith A.; Turner, Michelle C. (Jul 2014). "The epidemiology of glioma in adults: a "state of the science" review". Neuro-Oncology. 16 (7): 896–913. doi:10.1093/neuonc/nou087. ISSN 1523-5866. PMC 4057143. PMID 24842956.
^ "CDC – Women's Safety and Health Issues at Work: Job Area: Agriculture". www.cdc.gov. NIOSH Workplace Safety and Health. Retrieved 2015-06-20.
^ Adel Fahmideh M, Schwartzbaum J, Frumento P, Feychting M (June 2014). "Association between DNA repair gene polymorphisms and risk of glioma: A systematic review and meta-analysis". Neuro-oncology. 16 (6): 807–14. doi:10.1093/neuonc/nou003. PMC 4022225. PMID 24500421.
^ abc Bernstein C, Prasad AR, Nfonsam V, Bernstein H. (2013). DNA Damage, DNA Repair and Cancer, New Research Directions in DNA Repair, Prof. Clark Chen (Ed.), ISBN 978-953-51-1114-6, InTech, http://www.intechopen.com/books/new-research-directions-in-dna-repair/dna-damage-dna-repair-and-cancer
^ Cuozzo C, Porcellini A, Angrisano T, Morano A, Lee B, Di Pardo A, Messina S, Iuliano R, Fusco A (2007). "DNA damage, homology-directed repair, and DNA methylation". PLoS Genet. 3 (7): e110. doi:10.1371/journal.pgen.0030110. PMC 1913100. PMID 17616978.CS1 maint: Multiple names: authors list (link)
^ O'Hagan HM, Mohammad HP, Baylin SB (2008). "Double strand breaks can initiate gene silencing and SIRT1-dependent onset of DNA methylation in an exogenous promoter CpG island". PLoS Genet. 4 (8): e1000155. doi:10.1371/journal.pgen.1000155. PMC 2491723. PMID 18704159.CS1 maint: Multiple names: authors list (link)
^ Skiriute D, Vaitkiene P, Saferis V, Asmoniene V, Skauminas K, Deltuva VP, Tamasauskas A (2012). "MGMT, GATA6, CD81, DR4, and CASP8 gene promoter methylation in glioblastoma". BMC Cancer. 12: 218. doi:10.1186/1471-2407-12-218. PMC 3404983. PMID 22672670.
^ ab Spiegl-Kreinecker S, Pirker C, Filipits M, Lötsch D, Buchroithner J, Pichler J, Silye R, Weis S, Micksche M, Fischer J, Berger W (January 2010). "O6-Methylguanine DNA methyltransferase protein expression in tumor cells predicts outcome of temozolomide therapy in glioblastoma patients". Neuro-oncology. 12 (1): 28–36. doi:10.1093/neuonc/nop003. PMC 2940563. PMID 20150365.
^ Zhang W, Zhang J, Hoadley K, Kushwaha D, Ramakrishnan V, Li S, Kang C, You Y, Jiang C, Song SW, Jiang T, Chen CC (June 2012). "miR-181d: a predictive glioblastoma biomarker that downregulates MGMT expression". Neuro-oncology. 14 (6): 712–19. doi:10.1093/neuonc/nos089. PMC 3367855. PMID 22570426.
^ Chen HY, Shao CJ, Chen FR, Kwan AL, Chen ZP (April 2010). "Role of ERCC1 promoter hypermethylation in drug resistance to cisplatin in human gliomas". Int. J. Cancer. 126 (8): 1944–54. doi:10.1002/ijc.24772. PMID 19626585.
^ Narayanan L, Fritzell JA, Baker SM, Liskay RM, Glazer PM (April 1997). "Elevated levels of mutation in multiple tissues of mice deficient in the DNA mismatch repair gene Pms2". Proc. Natl. Acad. Sci. U.S.A. 94 (7): 3122–27. doi:10.1073/pnas.94.7.3122. PMC 20332. PMID 9096356.
^ Hegan DC, Narayanan L, Jirik FR, Edelmann W, Liskay RM, Glazer PM (December 2006). "Differing patterns of genetic instability in mice deficient in the mismatch repair genes Pms2, Mlh1, Msh2, Msh3 and Msh6". Carcinogenesis. 27 (12): 2402–08. doi:10.1093/carcin/bgl079. PMC 2612936. PMID 16728433.
^ Tutt AN, van Oostrom CT, Ross GM, van Steeg H, Ashworth A (March 2002). "Disruption of Brca2 increases the spontaneous mutation rate in vivo: synergism with ionizing radiation". EMBO Rep. 3 (3): 255–60. doi:10.1093/embo-reports/kvf037. PMC 1084010. PMID 11850397.
^ abc Molenaar, Remco J.; Radivoyevitch, Tomas; Maciejewski, Jaroslaw P.; van Noorden, Cornelis J. F.; Bleeker, Fonnet E. (2014-12-01). "The driver and passenger effects of isocitrate dehydrogenase 1 and 2 mutations in oncogenesis and survival prolongation". Biochimica et Biophysica Acta (BBA) - Reviews on Cancer. 1846 (2): 326–41. doi:10.1016/j.bbcan.2014.05.004. PMID 24880135.
^ ab Cohen AL, Holmen SL, Colman H (May 2013). "IDH1 and IDH2 mutations in gliomas". Curr Neurol Neurosci Rep. 13 (5): 345. doi:10.1007/s11910-013-0345-4. PMC 4109985. PMID 23532369.
^ Wang P, Dong Q, Zhang C, Kuan PF, Liu Y, Jeck WR, Andersen JB, Jiang W, Savich GL, Tan TX, Auman JT, Hoskins JM, Misher AD, Moser CD, Yourstone SM, Kim JW, Cibulskis K, Getz G, Hunt HV, Thorgeirsson SS, Roberts LR, Ye D, Guan KL, Xiong Y, Qin LX, Chiang DY (June 2013). "Mutations in isocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholangiocarcinomas and share hypermethylation targets with glioblastomas". Oncogene. 32 (25): 3091–100. doi:10.1038/onc.2012.315. PMC 3500578. PMID 22824796.
^ Toyota M, Ahuja N, Ohe-Toyota M, Herman JG, Baylin SB, Issa JP (July 1999). "CpG island methylator phenotype in colorectal cancer". Proc. Natl. Acad. Sci. U.S.A. 96 (15): 8681–86. doi:10.1073/pnas.96.15.8681. PMC 17576. PMID 10411935.
^ Mojarad EN, Kuppen PJ, Aghdaei HA, Zali MR (2013). "The CpG island methylator phenotype (CIMP) in colorectal cancer". Gastroenterol Hepatol Bed Bench. 6 (3): 120–28. PMC 4017514. PMID 24834258.
^ Molenaar, Remco J.; Botman, Dennis; Smits, Myrthe A.; Hira, Vashendriya V.; Lith, Sanne A. van; Stap, Jan; Henneman, Peter; Khurshed, Mohammed; Lenting, Krissie (2015-11-15). "Radioprotection of IDH1-Mutated Cancer Cells by the IDH1-Mutant Inhibitor AGI-5198". Cancer Research. 75 (22): 4790–802. doi:10.1158/0008-5472.CAN-14-3603. ISSN 0008-5472. PMID 26363012.
^ Watanabe T, Nobusawa S, Kleihues P, Ohgaki H (April 2009). "IDH1 mutations are early events in the development of astrocytomas and oligodendrogliomas". Am. J. Pathol. 174 (4): 1149–53. doi:10.2353/ajpath.2009.080958. PMC 2671348. PMID 19246647.
^ von Deimling A, Eibl RH, Ohgaki H, Louis DN, von Ammon K, Petersen I, Kleihues P, Chung RY, Wiestler OD, Seizinger BR (1992). "p53 mutations are associated with 17p allelic loss in grade II and grade III astrocytoma". Cancer Research. 52 (10): 2987–90. PMID 1349850.
^ Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W, Kos I, Batinic-Haberle I, Jones S, Riggins GJ, Friedman H, Friedman A, Reardon D, Herndon J, Kinzler KW, Velculescu VE, Vogelstein B, Bigner DD (19 Feb 2009). "IDH1 and IDH2 mutations in gliomas". N Engl J Med. 360 (8): 765–73. doi:10.1056/NEJMoa0808710. PMC 2820383. PMID 19228619.
^ Wong ET, Brem S (2007). "Taming glioblastoma: targeting angiogenesis". J. Clin. Oncol. 25 (30): 4705–06. doi:10.1200/JCO.2007.13.1037. PMID 17947716.
^ ab Jiang, Bowen; Chaichana, Kaisorn; Veeravagu, Anand; Chang, Steven D.; Black, Keith L.; Patil, Chirag G. (2017-04-27). "Biopsy versus resection for the management of low-grade gliomas". The Cochrane Database of Systematic Reviews. 4: CD009319. doi:10.1002/14651858.CD009319.pub3. ISSN 1469-493X. PMID 28447767.
^ Metcalfe, S. E.; Grant, R. (2001). "Biopsy versus resection for malignant glioma". The Cochrane Database of Systematic Reviews (3): CD002034. doi:10.1002/14651858.CD002034. ISSN 1469-493X. PMID 11687008.
^ Stewart L, Burdett S; Glioma Meta-analysis Trialists Group (GMT) (2002). Stewart, Lesley, ed. "Chemotherapy for high-grade glioma". Cochrane Database Syst Rev (3): CD003913. doi:10.1002/14651858.CD003913. PMID 12519620.CS1 maint: Multiple names: authors list (link)
^ abc Hart, Michael G.; Garside, Ruth; Rogers, Gabriel; Stein, Ken; Grant, Robin (2013-04-30). "Temozolomide for high grade glioma". The Cochrane Database of Systematic Reviews (4): CD007415. doi:10.1002/14651858.CD007415.pub2. ISSN 1469-493X. PMID 23633341.
^ Johnson BE, Mazor T, Hong C; et al. (2014). "Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma". Science. 343 (6167): 189–93. doi:10.1126/science.1239947. PMC 3998672. PMID 24336570. Retrieved 17 June 2015.CS1 maint: Explicit use of et al. (link) CS1 maint: Multiple names: authors list (link)
^ "Recurrent Brain Cancers Follow Distinctive Genetic Paths". University of California Santa Cruz. University of California San Francisco. Retrieved 17 June 2015.
^ Rob Stein (May 20, 2008). "Malignant Gliomas Affect About 10,000 Americans Annually". Washington Post.
^ ab Smoll, N. R.; Gautschi, O. P.; Schatlo, B.; Schaller, K.; Weber, D. C. (2012). "Relative survival of patients with supratentorial low-grade gliomas". Neuro-Oncology. 14 (8): 1062–69. doi:10.1093/neuonc/nos144. ISSN 1522-8517. PMC 3408266.
^ Ohgaki H, Kleihues P (June 2005). "Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas". J Neuropathol Exp Neurol. 64 (6): 479–89. PMID 15977639.
^ http://www.neurology.org/cgi/content/abstract/54/7/1442
^ Bleeker, Fonnet E.; Molenaar, Remco J.; Leenstra, Sieger (2012-01-20). "Recent advances in the molecular understanding of glioblastoma". Journal of Neuro-Oncology. 108 (1): 11–27. doi:10.1007/s11060-011-0793-0. ISSN 0167-594X. PMC 3337398. PMID 22270850.
^ "Archived copy". Archived from the original on 2014-05-02. Retrieved 2014-05-01.CS1 maint: Archived copy as title (link)
^ Kebudi R, Cakir FB (Oct 2013). "Management of diffuse pontine gliomas in children: recent developments". Paediatr Drugs. 15 (5): 351–62. doi:10.1007/s40272-013-0033-5. PMID 23719782.
^ Fisher PG, Breiter SN, Carson BS, Wharam MD, Williams JA, Weingart JD, Foer DR, Goldthwaite PT, Burger PC (2000). "A clinicopathologic reappraisal of brainstem tumor classification: identification of pilocytic astrocytoma and fibrillary astrocytoma as distinct entities". Cancer. 89: 1569–76. doi:10.1002/1097-0142(20001001)89:7<1569::aid-cncr22>3.0.co;2-0.
^ Donaldson SS, Laningham F, Fisher PG (2006). "Advances toward an understanding of brain stem gliomas". J Clin Oncol. 24: 1266–72. doi:10.1200/jco.2005.04.6599.
^ Jansen MH, van Vuurden DG, Vandertop WP, Kaspers GJ (Feb 2012). "Diffuse intrinsic pontine gliomas: a systematic update on clinical trials and biology". Cancer Treat Rev. 38 (1): 27–35. doi:10.1016/j.ctrv.2011.06.007. PMID 21764221.
^ Molenaar, Remco J.; Verbaan, Dagmar; Lamba, Simona; Zanon, Carlo; Jeuken, Judith W. M.; Boots-Sprenger, Sandra H. E.; Wesseling, Pieter; Hulsebos, Theo J. M.; Troost, Dirk (2014-09-01). "The combination of IDH1 mutations and MGMT methylation status predicts survival in glioblastoma better than either IDH1 or MGMT alone". Neuro-Oncology. 16 (9): 1263–73. doi:10.1093/neuonc/nou005. ISSN 1522-8517. PMC 4136888. PMID 24510240.
External links
| Classification | D
|
|---|
Glioma at the Human Protein Atlas- American Brain Tumor Association: Malignant Gliomas
- Brain and Spinal Tumors: Hope Through Research (National Institute of Neurological Disorders and Stroke)
- German Brain Tumor Association
- WHO Classification of Glioma
Glioma Images MedPix Database