Hysterectomy

 Clash Royale CLAN TAG#URR8PPP
Clash Royale CLAN TAG#URR8PPP
| Hysterectomy | |
|---|---|
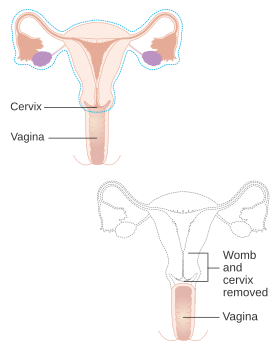 Diagram showing what is removed with a radical hysterectomy | |
| ICD-9-CM | 68.9 |
| MeSH | D007044 |
| MedlinePlus | 002915 |
Hysterectomy is the surgical removal of the uterus. It may also involve removal of the cervix, ovaries, fallopian tubes and other surrounding structures.
Usually performed by a gynecologist, a hysterectomy may be total (removing the body, fundus, and cervix of the uterus; often called "complete") or partial (removal of the uterine body while leaving the cervix intact; also called "supracervical"). It is the most commonly performed gynecological surgical procedure. In 2003, over 600,000 hysterectomies were performed in the United States alone, of which over 90% were performed for benign conditions.[1] Such rates being highest in the industrialized world has led to the major controversy that hysterectomies are being largely performed for unwarranted and unnecessary reasons.[2]
Removal of the uterus renders the patient unable to bear children (as does removal of ovaries and fallopian tubes) and has surgical risks as well as long-term effects, so the surgery is normally recommended when other treatment options are not available or have failed. It is expected that the frequency of hysterectomies for non-malignant indications will fall as there are good alternatives in many cases.[3]
Oophorectomy (removal of ovaries) is frequently done together with hysterectomy to decrease the risk of ovarian cancer. However, recent studies have shown that prophylactic oophorectomy without an urgent medical indication decreases a woman’s long-term survival rates substantially and has other serious adverse effects.[4][5] This effect is not limited to pre-menopausal women; even women who have already entered menopause were shown to have experienced a decrease in long-term survivability post-oophorectomy.[6]
Contents
1 Medical uses
1.1 Gynecological malignancies
1.2 Risks and adverse effects
1.3 Recovery
1.4 Unintended oophorectomy and premature ovarian failure
1.5 Effects on sexual life and pelvic pain
1.6 Premature menopause and its effects
1.7 Urinary incontinence and vaginal prolapse
1.8 Adhesion formation and bowel obstruction
1.9 Wound infection
1.10 Other rare problems
2 Alternatives
2.1 Heavy bleeding
2.2 Uterine fibroids
2.3 Prolapse
3 Types
4 Technique
4.1 Abdominal hysterectomy
4.2 Vaginal hysterectomy
4.3 Laparoscopic-assisted vaginal hysterectomy
4.4 Laparoscopic-assisted supracervical hysterectomy
4.5 Total laparoscopic hysterectomy
4.6 Other techniques
4.7 Comparison of techniques
5 Incidence
5.1 Canada
5.2 United States
5.3 United Kingdom
5.4 Germany
5.5 Denmark
6 See also
7 References
8 External links
Medical uses
Hysterectomy
Hysterectomy is a major surgical procedure that has risks and benefits, and affects a woman's hormonal balance and overall health for the rest of her life. Because of this, hysterectomy is normally recommended as a last resort to remedy certain intractable uterine/reproductive system conditions. Such conditions include, but are not limited to:
- Severe and intractable endometriosis (growth of the uterine lining outside the uterine cavity) and/or adenomyosis (a form of endometriosis, where the uterine lining has grown into and sometimes through the uterine wall musculature), after pharmaceutical or other surgical options have been exhausted.[7][8]
- Chronic pelvic pain, after pharmaceutical or other surgical options have been exhausted.[7][8]
Postpartum to remove either a severe case of placenta praevia (a placenta that has either formed over or inside the birth canal) or placenta percreta (a placenta that has grown into and through the wall of the uterus to attach itself to other organs), as well as a last resort in case of excessive obstetrical haemorrhage.[9]- Several forms of vaginal prolapse.[7][8]
Women may also express a desire to undergo an elective hysterectomy for reasons other than the resolution of reproductive system conditions or illnesses. Some of the conditions under which a person may request to have a hysterectomy (or have one requested for her if the woman is incapable of making the request) for non-illness reasons include may be as prophylaxis against certain reproductive system cancers, especially if there is a strong family history of reproductive system cancers (especially breast cancer in conjunction with BRCA1 or BRCA2 mutation), or as part of recovery from such cancers. Some with severe developmental disabilities have had hysterectomies though this treatment is controversial at best. In the United States, specific cases of sterilization due to developmental disabilities have been found by state-level Supreme Courts to violate the patient's constitutional and common law rights.[10]
Gynecological malignancies
Many types of reproductive system cancers are treated surgically. These include uterine, cervical, ovarian, or endometrium tumors, as well as uterine fibroids that do not respond to more conservative treatment options.[7]
Risks and adverse effects
In 1995, the short-term mortality (within 40 days of surgery) was reported at 0.38 cases per 1000 when performed for benign causes. Risks for surgical complications were presence of fibroids, younger age (vascular pelvis with higher bleeding risk and larger uterus), dysfunctional uterine bleeding and parity.[11]
The mortality rate is several times higher when performed in patients who are pregnant, have cancer or other complications.[12]
Long-term effect on all case mortality is relatively small. Women under the age of 45 years have a significantly increased long-term mortality that is believed to be caused by the hormonal side effects of hysterectomy and prophylactic oophorectomy.[4]
Approximately 35% of women after hysterectomy undergo another related surgery within 2 years.
Ureteral injury is not uncommon and occurs in 0.2 per 1,000 cases of vaginal hysterectomy and 1.3 per 1,000 cases of abdominal hysterectomy.[13] The injury usually occurs in the distal ureter close to the infundibulopelvic ligament or as a ureter crosses below the uterine artery, often from blind clamping and ligature placement to control hemorrhage.[14]
Recovery
Hospital stay is 3 to 5 days or more for the abdominal procedure and between 1 and 2 days (but possibly longer) for vaginal or laparoscopically assisted vaginal procedures.[15]
Unintended oophorectomy and premature ovarian failure
Removal of one or both ovaries is performed in a substantial number of hysterectomies that were intended to be ovary sparing.[16]
The average onset age of menopause after hysterectomy with ovarian conservation is 3.7 years earlier than average.[17] This has been suggested to be due to the disruption of blood supply to the ovaries after a hysterectomy or due to missing endocrine feedback of the uterus. The function of the remaining ovaries is significantly affected in about 40% of women, some of them even require hormone replacement treatment. Surprisingly, a similar and only slightly weaker effect has been observed for endometrial ablation which is often considered as an alternative to hysterectomy.
A substantial number of women develop benign ovarian cysts after a hysterectomy.[18]
Effects on sexual life and pelvic pain
After hysterectomy for benign indications the majority of women report improvement in sexual life and pelvic pain. A smaller share of women report worsening of sexual life and other problems. The picture is significantly different for hysterectomy performed for malignant reasons; the procedure is often more radical with substantial side effects.[19][20] A proportion of patients who undergo a hysterectomy for chronic pelvic pain continue to suffer from pelvic pain after a hysterectomy and develop dyspareunia (painful sexual intercourse).[21]
Premature menopause and its effects
Estrogen levels fall sharply when the ovaries are removed, removing the protective effects of estrogen on the cardiovascular and skeletal systems. This condition is often referred to as "surgical menopause", although it is substantially different from a naturally occurring menopausal state; the former is a sudden hormonal shock to the body that causes rapid onset of menopausal symptoms such as hot flashes, while the latter is a gradually occurring decrease of hormonal levels over a period of years with uterus intact and ovaries able to produce hormones even after the cessation of menstrual periods.
One study showed that risk of subsequent cardiovascular disease is substantially increased for women who had hysterectomy at age 50 or younger. No association was found for women undergoing the procedure after age 50. The risk is higher when ovaries are removed but still noticeable even when ovaries are preserved.[22]
Several other studies have found that osteoporosis (decrease in bone density) and increased risk of bone fractures are associated with hysterectomies.[23][24][25][26][27][28] This has been attributed to the modulatory effect of estrogen on calcium metabolism and the drop in serum estrogen levels after menopause can cause excessive loss of calcium leading to bone wasting.
Hysterectomies have also been linked with higher rates of heart disease and weakened bones. Those who have undergone a hysterectomy with both ovaries removed typically have reduced testosterone levels as compared to those left intact.[16] Reduced levels of testosterone in women are predictive of height loss, which may occur as a result of reduced bone density,[29] while increased testosterone levels in women are associated with a greater sense of sexual desire.[30]
Oophorectomy before the age of 45 is associated with a fivefold mortality from neurologic and mental disorders.[31]
Urinary incontinence and vaginal prolapse
Urinary incontinence and vaginal prolapse are well known adverse effects that develop with high frequency a very long time after the surgery. Typically, those complications develop 10–20 years after the surgery.[32] For this reason exact numbers are not known, and risk factors are poorly understood. It is also unknown if the choice of surgical technique has any effect. It has been assessed that the risk for urinary incontinence is approximately doubled within 20 years after hysterectomy. One long-term study found a 2.4 fold increased risk for surgery to correct urinary stress incontinence following hysterectomy.[33][34]
The risk for vaginal prolapse depends on factors such as number of vaginal deliveries, the difficulty of those deliveries, and the type of labor.[35] Overall incidence is approximately doubled after hysterectomy.[36]
Adhesion formation and bowel obstruction
The formation of postoperative adhesions is a particular risk after hysterectomy because of the extent of dissection involved as well as the fact the hysterectomy wound is in the most gravity-dependent part of the pelvis into which a loop of bowel may easily fall.[37] In one review, incidence of small bowel obstruction due to intestinal adhesion was found to be 15.6% in non-laparoscopic total abdominal hysterectomies vs. 0.0% in laparoscopic hysterecomies.[38]
Wound infection
Wound infection occurs in approximately 3% of cases of abdominal hysterectomy. The risk is increased by obesity, diabetes, immunodeficiency disorder, use of systemic corticosteroids, smoking, wound hematoma, and preexisting infection such as chorioamnionitis and pelvic inflammatory disease.[39] Such wound infections mainly take the form of either incisional abscess or wound cellulitis. Typically, both confer erythema, but only an incisional abscess confers purulent drainage. The recommended treatment of an incisional abscess after hysterectomy is by incision and drainage, and then coverage by a thin layer of gauze followed by sterile dressing. The dressing should be changed and the wound irrigated with normal saline at least twice each day. In addition, it is recommended to administer an antibiotic active against staphylococci and streptococci, preferably vancomycin when there is a risk of MRSA.[39] The wound can be allowed to close by secondary intention. Alternatively, if the infection is cleared and healthy granulation tissue is evident at the base of the wound, the edges of the incision may be reapproximated, such as by using butterfly stitches, staples or sutures.[39] Sexual intercourse remains possible after hysterectomy. Reconstructive surgery remains an option for women who have experienced benign and malignant conditions.[40]:1020–1348
Other rare problems
Hysterectomy may cause an increased risk of the relatively rare renal cell carcinoma. The increased risk is particularly pronounced for young women; the risk was lower after vaginally performed hysterectomies.[41] Hormonal effects or injury of the ureter were considered as possible explanations.[42][43] In some cases the renal cell carcinoma may be a manifestation of an undiagnosed hereditary leiomyomatosis and renal cell cancer syndrome.
Removal of the uterus without removing the ovaries can produce a situation that on rare occasions can result in ectopic pregnancy due to an undetected fertilization that had yet to descend into the uterus before surgery. Two cases have been identified and profiled in an issue of the Blackwell Journal of Obstetrics and Gynecology; over 20 other cases have been discussed in additional medical literature.[44] There is possibly another case of ectopic pregnancy after hysterectomy that took place in 2016, although no additional information has been brought forward. On very rare occasions, sexual intercourse after hysterectomy may cause a transvaginal evisceration of the small bowel.[45] The vaginal cuff is the uppermost region of the vagina that has been sutured close. A rare complication, it can dehisce and allow the evisceration of the small bowel into the vagina.[46]
Alternatives

Myomectomy

Sutured uterus wound after myomectomy
Depending on the indication there are alternatives to hysterectomy :
Heavy bleeding
Levonorgestrel intrauterine devices are highly effective at controlling dysfunctional uterine bleeding (DUB) or menorrhagia and should be considered before any surgery.[47]
Menorrhagia (heavy or abnormal menstrual bleeding) may also be treated with the less invasive endometrial ablation which is an outpatient procedure in which the lining of the uterus is destroyed with heat, mechanically or by radio frequency ablation. Endometrial ablation greatly reduces or entirely eliminates monthly bleeding in ninety percent of patients with DUB. It is not effective for patients with very thick uterine lining or uterine fibroids.[48]
Uterine fibroids
Levonorgestrel intrauterine devices are highly effective in limiting menstrual blood flow and improving other symptoms. Side effects are typically very moderate because the levonorgestrel (a progestin) is released in low concentration locally. There is now substantial evidence that Levongestrel-IUDs provide good symptomatic relief for women with fibroids.[49]
Uterine fibroids may be removed and the uterus reconstructed in a procedure called "myomectomy." A myomectomy may be performed through an open incision, laparoscopically or through the vagina (hysterescopy).[50]
Uterine artery embolization (UAE) is a minimally invasive procedure for treatment of uterine fibroids. Under local anesthesia a catheter is introduced into the femoral artery at the groin and advanced under radiographic control into the uterine arterty. A mass of microspheres or polyvinyl alcohol (PVA) material (an embolus) is injected into the uterine arteries in order to block the flow of blood through those vessels. The restriction in blood supply usually results in significant reduction of fibroids and improvement of heavy bleeding tendency. The 2012 Cochrane review comparing hysterectomy and UAE did not find any major advantage for either procedure. While UAE is associated with shorter hospital stay and a more rapid return to normal daily activities, it was also associated with a higher risk for minor complications later on. There were no differences between UAE and hysterectomy with regards to major complications.[51]
Uterine fibroids can be removed with a non-invasive procedure called Magnetic Resonance guided Focused Ultrasound (MRgFUS).
Prolapse
Prolapse may also be corrected surgically without removal of the uterus.[52]
Types

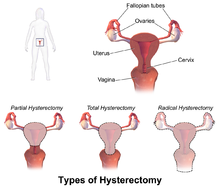
Schematic drawing of types of hysterectomy
Hysterectomy, in the literal sense of the word, means merely removal of the uterus. However other organs such as ovaries, fallopian tubes and the cervix are very frequently removed as part of the surgery.
Radical hysterectomy: complete removal of the uterus, cervix, upper vagina, and parametrium. Indicated for cancer. Lymph nodes, ovaries and fallopian tubes are also usually removed in this situation, such as in Wertheim's hysterectomy.[53]
Total hysterectomy: complete removal of the uterus and cervix, with or without oophorectomy.
Subtotal hysterectomy: removal of the uterus, leaving the cervix in situ.
Subtotal (supracervical) hysterectomy was originally proposed with the expectation that it may improve sexual functioning after hysterectomy, it has been postulated that removing the cervix causes excessive neurologic and anatomic disruption, thus leading to vaginal shortening, vaginal vault prolapse, and vaginal cuff granulations. These theoretical advantages were not confirmed in practice, but other advantages over total hysterectomy emerged. The principal disadvantage is that risk of cervical cancer is not eliminated and women may continue cyclical bleeding (although substantially less than before the surgery).
These issues were addressed in a systematic review of total versus supracervical hysterectomy for benign gynecological conditions, which reported the following findings:[54]
- There was no difference in the rates of incontinence, constipation, measures of sexual function or alleviation of pre-surgery symptoms.
- Length of surgery and amount of blood lost during surgery were significantly reduced during supracervical hysterectomy compared to total hysterectomy, but there was no difference in post-operative transfusion rates.
- Febrile morbidity was less likely and ongoing cyclic vaginal bleeding one year after surgery was more likely after supracervical hysterectomy.
- There was no difference in the rates of other complications, recovery from surgery, or readmission rates.
In the short-term, randomized trials have shown that cervical preservation or removal does not affect the rate of subsequent pelvic organ prolapse.[55]
Supracervical hysterectomy does not eliminate the possibility of having cervical cancer since the cervix itself is left intact and may be contraindicated in women with increased risk of this cancer; regular pap smears to check for cervical dysplasia or cancer are still needed.[56][57]
Technique
Hysterectomy can be performed in different ways. The oldest known technique is vaginal hysterectomy. The first planned hysterectomy was performed by Konrad Langenbeck - Surgeon General of the Hannovarian army, although there are records of vaginal hysterectomy for prolapse going back as far as 50BC.
The first abdominal hysterectomy recorded was by Ephraim McDowell. He performed the procedure in 1809 for a mother of five for a large ovarian mass on her kitchen table.[58]
In modern medicine today, laparoscopic vaginal (With additional instruments passing through ports in small abdominal incisions, close or in the navel) and total laparoscopic techniques have been developed.
Abdominal hysterectomy
Most hysterectomies in the United States are done via laparotomy (abdominal incision, not to be confused with laparoscopy). A transverse (Pfannenstiel) incision is made through the abdominal wall, usually above the pubic bone, as close to the upper hair line of the individual's lower pelvis as possible, similar to the incision made for a caesarean section. This technique allows physicians the greatest access to the reproductive structures and is normally done for removal of the entire reproductive complex. The recovery time for an open hysterectomy is 4–6 weeks and sometimes longer due to the need to cut through the abdominal wall. Historically, the biggest problem with this technique was infections, but infection rates are well-controlled and not a major concern in modern medical practice. An open hysterectomy provides the most effective way to explore the abdominal cavity and perform complicated surgeries. Before the refinement of the vaginal and laparoscopic vaginal techniques, it was also the only possibility to achieve subtotal hysterectomy; meanwhile, the vaginal route is the preferable technique in most circumstances.[59][60]
Vaginal hysterectomy
Vaginal hysterectomy is performed entirely through the vaginal canal and has clear advantages over abdominal surgery such as fewer complications, shorter hospital stays and shorter healing time. Abdominal hysterectomy, the most common method, is used in cases such as after caesarean delivery, when the indication is cancer, when complications are expected, or surgical exploration is required.
Laparoscopic-assisted vaginal hysterectomy
With the development of laparoscopic techniques in the 1970s and 1980s, the "laparoscopic-assisted vaginal hysterectomy" (LAVH) has gained great popularity among gynecologists because compared with the abdominal procedure it is less invasive and the post-operative recovery is much faster. It also allows better exploration and slightly more complicated surgeries than the vaginal procedure. LAVH begins with laparoscopy and is completed such that the final removal of the uterus (with or without removing the ovaries) is via the vaginal canal. Thus, LAVH is also a total hysterectomy; the cervix is removed with the uterus.[61] If the cervix is removed along with the uterus, the upper portion of the vagina is sutured together and called the vaginal cuff.[62]
Laparoscopic-assisted supracervical hysterectomy
The "laparoscopic-assisted supracervical hysterectomy" (LASH) was later developed to remove the uterus without removing the cervix using a morcellator which cuts the uterus into small pieces that can be removed from the abdominal cavity via the laparoscopic ports.
Total laparoscopic hysterectomy
Total laparoscopic hysterectomy (TLH) was developed in the early 90s by Prabhat K. Ahluwalia in Upstate New York.[63] TLH is performed solely through the laparoscopes in the abdomen, starting at the top of the uterus, typically with a uterine manipulator. The entire uterus is disconnected from its attachments using long thin instruments through the "ports". Then all tissue to be removed is passed through the small abdominal incisions.
Other techniques
Supracervical (subtotal) laparoscopic hysterectomy (LSH) is performed similar to the total laparoscopic surgery but the uterus is amputated between the cervix and fundus.
Dual-port laparoscopy is a form of laparoscopic surgery using two 5 mm midline incisions: the uterus is detached through the two ports and removed through the vagina.[64][65]
"Robotic hysterectomy" is a variant of laparoscopic surgery using special remotely controlled instruments that allow the surgeon finer control as well as three-dimensional magnified vision.[66]

Uterus prior to hysterectomy

Laparoscopical hysterectomy

Cervical stump (white) after removal of the uterine corpus at laparoscopic supracervical hysterectomy

Transvaginal extraction of the uterus in total laparoscopical hysterectomy

End of an laparoscopical hysterectomy





Comparison of techniques
Patient characteristics such as the reason for needing a hysterectomy, uterine size, descent of the uterus, presence of diseased tissues surrounding the uterus, previous surgery in the pelvic region, obesity, history of pregnancy, the possibility of endometriosis, or the need for an oophorectomy, will influence a surgeon’s surgical approach when performing a hysterectomy.[67]
Vaginal hysterectomy is recommended over other variants where possible for women with benign diseases.[59][60][67] Vaginal hysterectomy was shown to be superior to LAVH and some types of laparoscopic surgery causing fewer short- and long-term complications, more favorable effect on sexual experience with shorter recovery times and fewer costs.[68][69][70]
Laparoscopic surgery offers certain advantages when vaginal surgery is not possible but also has the disadvantage of significantly longer time required for the surgery.[67]
In one 2004 study conducted in the UK comparing abdominal (laparotomic) and laparoscopic techniques, laparoscopic surgery was found to cause longer operation time and a higher rate of major complications while offering much quicker healing.[71] In another study conducted in 2014, laparoscopy was found to be "a safe alternative to laparotomy" in patients receiving total hysterectomy for endometrial cancer. Researchers concluded the procedure "offers markedly improved perioperative outcomes with a lower reoperation rate and fewer postoperative complications when the standard of care shifts from open surgery to laparoscopy in a university hospital".[72]
Vaginal hysterectomy is the only available option that is feasible without total anaesthesia or in outpatient settings (although doing it without anesthesia is recommended only in exceptional cases).[citation needed]
The abdominal technique is very often applied in difficult circumstances or when complications are expected. Given these circumstances the complication rate and time required for surgery compares very favorably with other techniques, however time required for healing is much longer.[67]
Hysterectomy by abdominal laparotomy is correlated with much higher incidence of intestinal adhesions than other techniques.[38]
Time required for completion of surgery in the eVAL trial is reported as follows:[71]
- abdominal 55.2 minutes average, range 19–155
- vaginal 46.6 minutes average, range 14–168
- laparoscopic (all variants) 82.5 minutes average, range 10–325 (combined data from both trial arms)
Morcellation has been widely used especially in laparoscopic techniques and sometimes for the vaginal technique, but now appears to be associated with a considerable risk of spreading benign or malignant tumors.[73][74] In April 2014, the FDA issued a memo alerting medical practitioners to the risks of power morcellation.[75]
Robotic assisted surgery is presently used in several countries for hysterectomies. Additional research is required to determine the benefits and risks involved, compared to conventional laparoscopic surgery.[76]
A 2014 Cochrane review found that robotic assisted surgery may have a similar complication rate when compared to conventional laparoscopic surgery. In addition, there is evidence to suggest that although the surgery make take longer, robotic assisted surgery may result in shorter hospital stays.[76] More research is necessary to determine if robotic assisted hysterectomies are beneficial for people with cancer.[76]
Previously reported marginal advantages of robotic assisted surgery could not be confirmed; only differences in hospital stay and cost remain statistically significant.[77][78][79][80][81] In addition, concerns over widespread misleading marketing claims have been raised.[82]
| Technique | Benefits | Disadvantages |
|---|---|---|
| Abdominal hysterectomy |
|
|
| Vaginal hysterectomy |
|
|
| Laparoscopic supracervical hysterectomy (subtotal hysterectomy) |
|
|
| Laparoscopic-assisted vaginal hysterectomy (LAVH) |
|
|
| Total laparoscopic hysterectomy |
|
|
| Single-port laparoscopic hysterectomy / mini laparoscopic hysterectomy |
| |
| Robotic-assisted hysterectomy |
|
|
Authority control |
|
|---|